N6) Ventilator dependence 1 week after MVC
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with altered mental status.
- Review the DDx considerations in a patient with altered mental status.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with altered mental status.
History
Physical Exam
Labs
Provisional Diagnosis
Potential Acuity
What is your assessment of the likely acuity for this patient?
First Imaging Study
What is the first imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
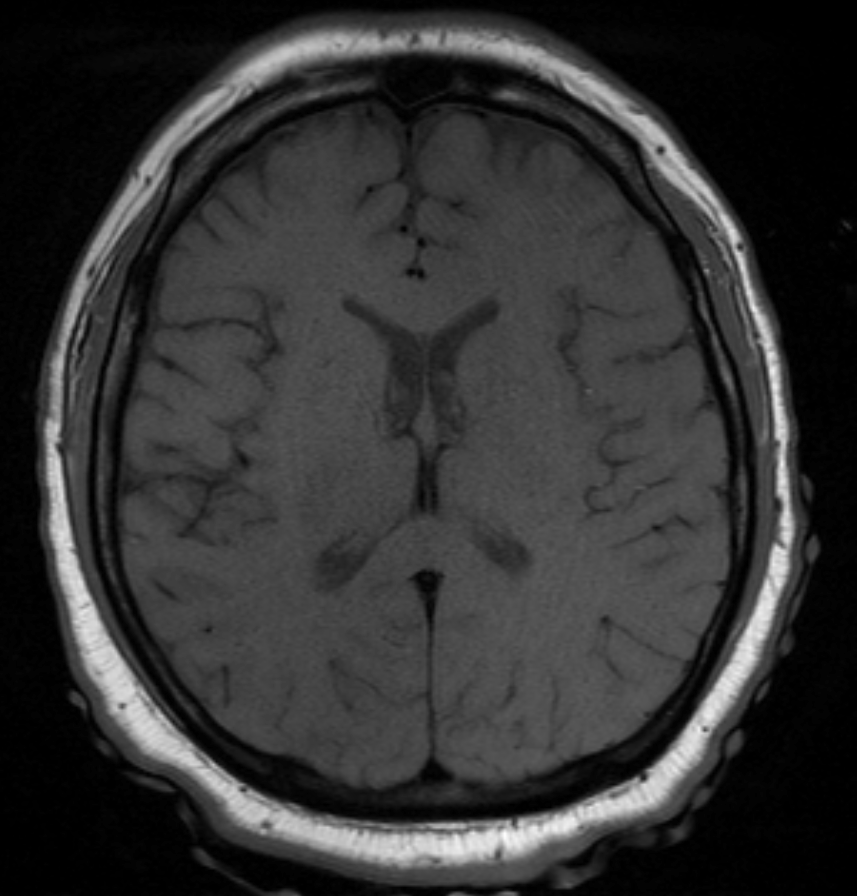
MRI head with and without contrast
There is evidence of cerebral edema.
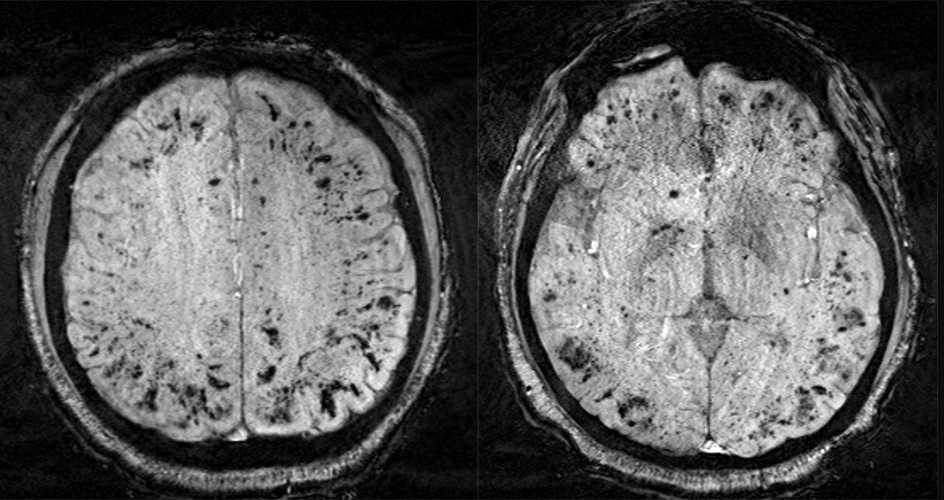
There are abnormal lesions.

Watch our video
Second Imaging Study
What is the next imaging study you will order?
What is your Diagnosis now that you have seen the imaging results?
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
Assessment and Plan
Please provide your assessment and plan for this patient
Lessons Learned:
- Diffuse axonal injury (DAI) occurs due to the shearing forces exerted on axons in the white matter as a result of rapid acceleration, deceleration, or rotational forces at the moment of injury.
- This injury often manifests with loss of consciousness, post-traumatic coma, and dysautonomic symptoms.
- The characteristic distribution of lesions in DAI commonly involves the gray-white junction and the corpus callosum. In more severe instances, there may also be brain stem involvement.
- Given the nature of DAI, initial clinical presentation can be challenging to diagnose using a CT scan, which may yield negative results. Therefore, an MRI is the preferred imaging modality for detecting and assessing suspected cases of DAI.
- DAI management is primarily focused on providing supportive care, prevention of secondary injuries, and neurorehabilitation.
- In patients presenting with a GCS of 8 or lower, intubation and mechanical ventilation are necessary, as these individuals are at increased risk of airway obstruction. The absence of a gag reflex in such cases poses a heightened risk of aspiration, while involvement of the brainstem can compromise respiratory drive and increase the risk of hypoxia.
- Developing cerebral edema is a common occurrence following a traumatic brain injury (TBI), and when severe, it may cause elevated intracranial pressure (ICP), a life-threatening situation that could potentially lead to brain herniation.
- In patients requiring prolonged mechanical ventilation, early intervention with tracheostomy and percutaneous endoscopic gastrostomy (PEG) tube placement can improve patient outcomes.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.

{kind=link}
{kind=link}